
Daily, the USA healthcare providers leave potential income on the table – not just because they delivered poor care, but because of avoidable coding errors. Nowadays complicated repayment landscape, precise medical coding is not a back-office function. It is the financial engine of your business, hospital, or health system.
Whether you are a solo physician in Texas, a multi-talented group in New York, or any regional hospital network in the Midwest, our AAPC and AHIMA – certified clinical coders are ready to support you in capturing each dollar you have earned – while staying completely compliant with ICD-10, CPT, HCPCS, and payer-specific instructions.
The American Medical Association estimates that US healthcare providers collectively lose over $125 billion annually because of improper billing and coding mistakes. Outsourcing to expert coders is one of the fastest, most affordable ways to recover that revenue.
There is no insufficiency of medical billing service vendors in the market. Here is what sets our experts apart:

Medical coding is the procedure of interpreting the medical documentation – diagnoses, procedures, and medical billing services – into standardized alphanumeric codes. These codes drive insurance claims, estimate repayment rates, and form the backbone of your whole income cycle. In the United States, coding precision directly influences 3 critical regions of your practice:
Undercoding outcomes in reducing repayments. Overcoding includes the risks of add-ons, penalties, and even fraud allegations under the False Claims Act.
Payers involving Medicare, Medicaid, and commercial insurers reject the claims with incorrect or unsupported codes. Every denial will include an administrative burden and delay payment by weeks or months.
The Office of Inspector General (OIG) actively monitors coding patterns for anomalies. HIPAA requires that all individuals’ data handled during the coding workflows be guarded under limited security protocols.
Staffing in-house coders adds another layer of severity. Certified coders are in short supply across the USA, and turnover is a bit higher. Training, certification revival, salaries, and advantages for even a small coding team that can easily exceed $200,000 per year – without any guarantee of precision or specialty coverage.
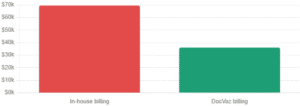
The numbers speak for themselves. For a business collecting $100,000 per month, here are the in-house coding prices as compared to outsourcing medical coding services to DocVaz:
Cost Factors | In-house Billing | DocVaz (per $100k collections) |
Annual staff salary | $54,480+ | Included in service |
Overhead & benefits | $15,000+ | $0 |
Software & HER | $3,000 – $12,000 / yr | Free EHR involved |
Training & Certification | $2000 – $5,000 / yr | $0 |
Total annual price | $69,480 | $ 35,998 |
Annual savings | – | Upto $33,482 |
Outsourcing medical coding services to DocVaz saves most practices $30,000 – $35,000 per year. While providing higher precision, quick turnaround, and built-in compliance. No hiring, no training, no turnover.
DocVaz Medical Billing Company offers a comprehensive range of medical coding services designed to integrate seamlessly with your existing workflows, practice management software, and EHR systems. Our facilities cover each care setting and specialty:
Services | Description |
Inpatient Coding | DRG examination and ICD-10-CM / PCS coding for hospital stays and admissions. |
Outpatient & Physician Coding | CPT and E&M coding for clinics, group practices, and outpatient departments. |
Specialty-Specific Coding | Addressed coding for cardiology, oncology, radiology, orthopedics, and behavioural health. |
HCC Complication Adjustment | Hierarchical condition category coding for Medicare benefits and value-based care contracts. |
Coding Audits | Prospective and retrospective audits to detect revenue leakage and compliance gaps. |
Emergency & Urgent Care | Fast-turnaround coding for high-volume ED and urgent care settings. |
Every arrangement starts with a thorough assessment of your current coding processes, payer mix, and documentation practices, so we can easily create a personalized coding plan, not a one-size-fits-all solution.
Let’s have a look at our company’s performance, whether in outcome breakdown and its effect:
Here is our proven and systematic strategy to represent patients’ diagnostic documentation within the codes:

Our certified coders are proficient in each main code set employed all over the USA healthcare settings:
International Classification of Diseases, 10th Revision, Medical Modification. It is mostly used for diagnostic coding across all care settings in the US.
The procedure coding system is used exclusively for inpatient hospitals’ methods and DRG assessment.
Sustained by the AMA, it is employed for physicians and outpatient method coding. Our coders are especially skilled in the E&M level selection, which is between the most frequently audited regions.
Covers the supplies, durable medical technologies (DME), injectables, and facilities not captured by CPT codes.
Used by Medicare and many commercial payers for estimating inpatient repayment. Proper DRG examination is important to hospital income integrity.
Used in the Medicare benefits complexities adjustment. Precise HCC coding ensures your individuals’ true health burden is captured, which directly affects your payment programs.
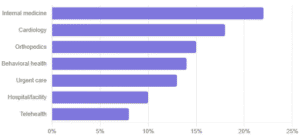
Each clinical specialty has its own coding way, payer quirks, and documentation needs. We provide you with a huge range of US healthcare providers, including:
If your specialty is not listed above, reach out; chances are we have certified coders with direct experience in your region.
Getting started is straightforward. Our onboarding method is designed to be quick, low-friction, and less disruptive to your existing workflow:
We start with a complimentary coding and documentation examination. Our expert coding team provides feedback on your current coding workflow, denial patterns, EHR setup, and payer mix. This provides us with an accurate picture of where income is being lost and where compliance complications exist.
Clinical analysis and documentation are shared through our HIPAA-compliant, encrypted file transfer platform. We sign a Business Associate Agreement (BAA) before any data exchange takes place, without any exceptions.
Our expert coders hold multiple CPC, CCS, CRC, or CDEO credentials - understanding the medical documentation, assigning suitable codes, and flagging any documentation insufficiency through a structured coder query method.
Each coded encounter goes through a multi-level QA method before submission, and we achieve a 95% precision rate and deliver your team with explained audit findings daily.
You get daily performance reports covering precise rates, denial trends, issues reactions times, and coder productivity. We employ this data to continually refine your coding plan and detect documentation enhancement opportunities.
Healthcare data is among the most sensitive across the world. We treat it that way. Every engagement is governed by a signed Business Associate Agreement (BAA) as needed under HIPAA. Our infrastructure uses AES-256 encryption for data at rest and in transit. Access to individuals’ records is role-based and limited to auditing. Staff experience annual HIPAA training, and all coders sign confidentiality agreements before managing your records.
We align our internal compliance plan with OIG instructions on billing and coding practices, and we conduct daily internal audits to detect and remediate any complication regions proactively – not reactively.
We never store your individual data on offshore servers. All data controlling happens within US-managed, HIPAA-compliant surroundings.
Knowing the price of medical coding services in the United States requires an examination of multiple cost models and specialty complexities. Most healthcare providers transition to outsourced models to convert high fixed prices into variable, performance-based expenditures.
Cost Category | Estimated Price Range (USD) |
Implementation & Setup | $1,000 – $20,000+ |
EHR/EMR Integration | $500 – $3,000 |
Staff Training | $150 – $500 per session |
Credentialing Fees | $100 – $500 per provider |
Software Maintenance | 15% – 20% of the initial cost |
Clearinghouse Fees | $30 – $100 per month |
Manual Claim Inquiries | $12 – $16 per inquiry |
Patient Statement Fees | $0.70 – $1.50 per statement |
Termination Fees | 1 – 3 months of service |
DocVaz serves Healthcare providers all over the nation. We have devoted billing and coding understanding to payer-specific needs. Medicaid rules and state-level compliance in every US state. Our higher volume markets involve:
Every location page involves certain state Medicaid billing rules, main payer details, and local provider resources. Meet our experts to describe your state’s specific coding needs.
Your medical team is providing excellent care. Make sure your coding reflects that – completely, precisely, and compliantly.
Partner with our US-related, AAPC and AHIMA-certified medical coders team and initiate recovering the income your practice has already earned. Whether you require complete outsourced coding aid, a one-time audit, or support covering a staffing gap, we have the best Medical Coding Services in the USA that adjust to your practice and your budget.
Contact DocVaz Medical Billing today for a free coding examination, and let’s have a look at exactly how much income your business could be leaving on the table. No commitment needed.
Most medical coding organizations charge either a per-chart fee (typically $1.50–$4.00 per encounter) or a percentage of collections (usually 2–5%). DocVaz offers transparent, personalized pricing based on your specialty, volume, and payer mix. There are no setup or additional fees.
Medical coding is the method of translating medical documentation into standardized codes (ICD-10, CPT, HCPCS). Medical billing employs those codes to create and submit claims to insurance payers, track unpaid claims, and manage denials. DocVaz delivers both facilities as part of an integrated revenue cycle management solution.
Look for coders certified by AAPC (CPC, CCS-P) or AHIMA (CCS, RHIA, CDEO). These credentials confirm proficiency in ICD-10, CPT, and HCPCS coding systems. All DocVaz coders hold at least one active AAPC or AHIMA credential and receive ongoing continuing education.
Certified coders understand every claim before submission, catching mismatched codes, missing modifiers, unsupported diagnoses, and documentation gaps — the top causes of first-pass rejections. DocVaz sustains a 95%+ first-pass precision rate and a 97% claim reimbursement rate.
Yes. DocVaz integrates seamlessly with all main EHR and practice management platforms, including Epic, Cerner, athenahealth, AdvancedMD, eClinicalWorks, Kareo, and others. Our onboarding team manages the technical setup — generally within 3–5 business days.
Most practices are fully onboarded within 5–7 business days. Our method includes a discovery call, documentation understandings, BAA signing, EHR integration, and a test batch of coded encounters prior to going live.
Yes, when performed correctly. DocVaz is fully HIPAA compliant. We sign a BAA with every client, use AES-256 encryption for all data, and process all patient records within a US-based, HIPAA-compliant infrastructure. Our internal compliance plan aligns with OIG instructions.